We are pleased to present our Q&A article with Roland Lyon, president of Kaiser Permanente (KP) of Colorado. In this role, Lyon leads the state’s largest nonprofit health plan, providing healthcare to approximately 670,000 members in Denver/Boulder, Southern Colorado, Northern Colorado, and the mountain communities of Summit and Eagle counties. Lyon joined KP in 2002, initially based in California before coming to Colorado in 2006. His roles in California included vice president of consulting and capital planning in KP’s Northern California region, and vice president of strategic planning in KP’s national program offices.
We are pleased to present our Q&A article with Roland Lyon, president of Kaiser Permanente (KP) of Colorado. In this role, Lyon leads the state’s largest nonprofit health plan, providing healthcare to approximately 670,000 members in Denver/Boulder, Southern Colorado, Northern Colorado, and the mountain communities of Summit and Eagle counties. Lyon joined KP in 2002, initially based in California before coming to Colorado in 2006. His roles in California included vice president of consulting and capital planning in KP’s Northern California region, and vice president of strategic planning in KP’s national program offices.
Key Takeaways
- Successful collaboration occurs when partners identify and align around overlapping interests.
- Making an effort to understand not only what is important to each partner but also why it is important allows for creative solutions to develop.
- A culture of collaboration must be modeled from the top to enlist leaders who are willing and able to collaborate across boundaries.
TLD Group: How do you define your health ecosystem?
Lyon: As a healthcare leader of an integrated health system, I define the health ecosystem in four concentric circles:
- The first circle is what I call the “inner circle” – the world that we directly control. This is the health insurance products, the care delivery teams (physician, nurses, etc.), etc. This is what one might consider traditional healthcare.
- The second circle includes our key partners who are contracted organizations and part of our broader he
althcare network, specifically providers such as hospitals and physician groups.
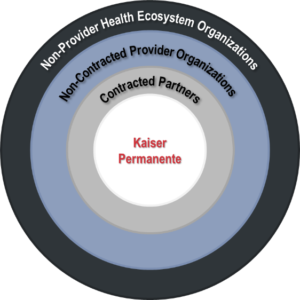 The third circle represents the “non-partnered” entrypoints into care. For example, this could be when someone finds themselves in a setting that’s not part of the plan. This could be considered other healthcare players that provide the more “reactive” sick care, like when you get into a car accident and are sent to the emergency room.
The third circle represents the “non-partnered” entrypoints into care. For example, this could be when someone finds themselves in a setting that’s not part of the plan. This could be considered other healthcare players that provide the more “reactive” sick care, like when you get into a car accident and are sent to the emergency room.- The fourth circle encompasses all of the non-healthcare provider members of the community. This could include elected officials, lawmakers and regulators, education systems, etc. In a broad sense, this circle represents any entity that impacts the health of the community.
TLD Group: What role do you think your organization plays in improving population health?
Lyon: KP understands that there are many drivers to the health of the community beyond simply providing healthcare. Some studies suggest that roughly 40% of the population’s health needs are determined by individual behaviors, 30% is attributable to environmental factors, 20% to traditional healthcare, and 10% is genetic. Since such a large percentage (40%) of the social determinants of health are driven by personal behaviors and lifestyle decisions. Along with incentivizing healthy choices, education plays a critical role in the health ecosystem. Given the provision of health care itself (i.e. treatment when sick), contributes so little to population health, we must pay attention to the other social determinants. As an example, KP supports and encourages its executives to serving on the boards of educational and other community health-minded institutions because we see education as a key driver of health, prevention, and wellness. To this end, KP has invested in an educational theater program, in which we employ several actors and actresses to go out into the community, often through the schools, to put on skits for students about healthy behaviors. One skit, called “Loose Change,” is based in a homeless shelter that’s serving dinner. The actors waiting in line for food are playing characters coming from all different backgrounds. One actress plays a woman who lost her job a year ago and can’t afford food because she still hasn’t found a new job. Another person is a veteran who has been injured, and earned the Purple Heart, but his pension gives only about $14 per week, which isn’t enough to afford food. The point of these skits is to educate the community about how the conditions people find themselves in, often out of their control, impact their health.
TLD Group: Can you provide an example of how your work in the inner circles of your health ecosystem has impacted the way you work with the outer circles?
Lyon: In Denver and Boulder, aside from hospitals, the delivery system is primarily owned by KP. The nurses are employed and we have dedicated Permanente physicians. We are able to offer enough volume and geographic access points so that care does not leak outside of the system. However, in smaller markets where the population is less dense, our ability to fulfill our mission is done in partnership with local hospitals and physicians. An example of this is our relatively recent expansion into Northern Colorado. To succeed as partners, we must have aligned financial, quality, and service objectives. It can be very complex as we try to work with those in the 3rd circle (non-partnered) to bring them into the 2nd circle (contracted). One organization, a healthcare organization operating in Northern Colorado, chose to contract with us because they saw us as a partner they could learn from and then apply those learnings to other markets where they operate. In this case, we brought our KP clinics to Northern Colorado, expanding capacity and access to critical primary care and other ambulatory services. These KP clinics with Colorado Permanente Medical Group physicians (CPMG – representing the 1st circle) are where we have our physicians and nurses and other care team members including pharmacy, lab, and imaging. We further contracted with this healthcare organization to provide additional primary care services at expanded geographic access points, as well as to generally provide specialty care services. We have approximately 60 community primary care physicians in our broader network (the 2nd circle), and we primarily deliver specialty care services to the insurance plan members through contracted specialty physician groups that are affiliated with the healthcare organization. What is a little unique and interesting is that we pay them on a budgeted fee-for-service basis that we reconcile at the end of the year and then share in the bottom line. This approach (until ultimately moving toward a full hospital capitated arrangement) has created aligned financial incentives, which has been a key part of our success in Northern Colorado because all parties are individually and collectively focused on health value – not volume and revenue.
TLD Group: How do you approach building relationships with partners in the health ecosystem?
Lyon: My approach is to understand their values, mission, and interests, to determine if they align with ours – which are to provide the best quality medicine to improve health. As a 501(3)(c) organization, KP is not beholden to shareholders. The owners of Kaiser Foundation of Colorado are effectively the citizens of Colorado. Because of this, KP can offer a more affordable product because we only need to make a 2% to 3% margin to meet our long-term financial objectives. As we improve the health of the communities we serve, it results in a lower cost structure, which transfers into lower insurance prices, and becomes something of a positive spiral. I look to find partners who share our interests. In my role, I have had to walk away from deals where interested were misaligned. One hospital company we spoke with was more driven by market share and revenue than by value. Another potential partner negotiated for a substantial increase to our rates. While they believed they should be able to increase their rates because they had the best quality and they did a lot of research, we did not agree. From my point of view, the lowest quality medicine is that which is unaffordable; the good news is that the most affordable care is that which is the highest quality, because it results in improved health, which in turn reduces the utilization of high-cost treatments.
TLD Group: How do you work through tension points to align on interests?
Lyon: It takes quite a bit of discussion, and requires that both parties articulate why they want what they are proposing, and not just the “what” itself. You have to dig deeper than the “what” to discover reasons that are aligned. It is only then that parties can work to find a solution that’s mutually beneficial. Of course, a degree of give-and-take also exists since we all have our different priorities. Both parties have to be willing to sacrifice a little, which can only occur when there is mutual respect, transparency, authenticity, willingness to listen, and a bit of humility. The last piece of it is just compromise, plain and simple. All of that is what it’s been like working with the healthcare organization in Northern Colorado. I think what finally tipped the scales on finalizing the contract with them was when we finally agreed to the financial approach, because then all of the negotiations not only unilaterally benefitted one party, they also benefit both through sharing of the bottom-line. Most importantly though is the sharing of and the commitment to improve the health of the communities we serve.
TLD Group: How do you drive consensus and collaboration within KP?
Lyon: I work with my team to determine our priorities – what’s most important to us. My top 5 priorities may be absolutely critical to me, whereas other priorities may be more open to a give-and-take. The other party’s top 5 might not be aligned with mine, but they may also have objectives that are more open to give-and-take as well. If you concede on one of your top priorities in order for the other party to have one of their priorities met, that goes a long way for building that relationship of trust. When they see that you are willing to give up something that is important to you for the bigger purpose of finding common ground, that strengthens the relationship. I try to get that point across to my team.
TLD Group: What is your approach to aligning processes between your organization and the partnering organization?
Lyon: We typically will defer to the subject matter experts. Oftentimes, when you let two peers (and especially two physicians) come together with their professional training and shared background, they almost always come back with something they both agree on. It’s not a negotiation as much as a discovery of what the right answers are using their shared expertise of best practices in the industry. It becomes somewhat like a puzzle where the collective effort creates a mutually agreed upon solution.
TLD Group: What role does KP play in collaborating with the broader health ecosystem, as opposed to the healthcare system?
Lyon: Regarding the 4th circle – which as I mentioned includes non-healthcare members of the health ecosystem – we have a lot of interaction with the community and educational institutions. But other players in that circle could include elected officials – those that are making and enforcing laws, and in general the regulatory environment. It is absolutely critical for a healthcare leader to be actively engaged with those elected officials – the governor’s office, the mayor’s office, the division of insurance commissioner, etc. – to help them fulfill their duty of creating a system for providing high-quality affordable healthcare access to all citizens in the state of Colorado. We’re becoming more and more regulated as an industry, in part because of our industry’s historical failure to deliver insurance and healthcare that is generally and consistently affordable. Working with policymakers has become a necessity to help educate and inform. Policymakers with the objective of “motivating” the health care industry players to deliver a more affordable product to more communities may make decisions that don’t fully deliver on the objective, or that have unintended negative consequences. Therefore, it is both in our interest as well as our obligation to be actively engaged in working with our elected officials and their teams – whether it’s the legislators who are making laws, or the regulators who implement and enforce those laws – to best understand the complex set of processes and relationships of the U.S. health care system. Some might wonder if it’s appropriate for a regulator to have a working relationship with those they’re regulating; I believe these interactions should be kept at an appropriate arm’s length. Yet I have observed on many occasions how working together brings better clarity to the issues, to potential options, which in turn results in the best decisions which support shared quality and affordability objectives.
View our other HELM Q&A Interviews:



 Andrew Baskin, MD, is Aetna’s Vice President, National MedicalDirector for Quality and Clinical Policy and served as the Interim Chief Medical Officer (in 2014). He works on initiatives to measure and improve quality of care, the provision of evidence based care, quality measurement implementation and public reporting, health plan accreditation, and the establishment of performance based networks. Additionally, Andy partners with others to help establish programs which create incentives for more effective and efficient care, influence and assure compliance with healthcare reform regulations, develop products to improve affordability and quality of care, and promote payment reform.
Andrew Baskin, MD, is Aetna’s Vice President, National MedicalDirector for Quality and Clinical Policy and served as the Interim Chief Medical Officer (in 2014). He works on initiatives to measure and improve quality of care, the provision of evidence based care, quality measurement implementation and public reporting, health plan accreditation, and the establishment of performance based networks. Additionally, Andy partners with others to help establish programs which create incentives for more effective and efficient care, influence and assure compliance with healthcare reform regulations, develop products to improve affordability and quality of care, and promote payment reform. Mohamed Diab, MD, Vice President of Provider Transformation leads population health management at Aetna. His focus is on providers as they transform their care delivery to achieve the “Triple Aim” by improving quality of care and reducing unnecessary cost. Mohamed has more than 25 years of experience as a provider as well as an executive in the payer and consulting industries. He has a background in medical management, pharmacy benefit management, clinical informatics and cost management programs.
Mohamed Diab, MD, Vice President of Provider Transformation leads population health management at Aetna. His focus is on providers as they transform their care delivery to achieve the “Triple Aim” by improving quality of care and reducing unnecessary cost. Mohamed has more than 25 years of experience as a provider as well as an executive in the payer and consulting industries. He has a background in medical management, pharmacy benefit management, clinical informatics and cost management programs.







 Robert C. Garrett is Co-CEO of Hackensack Meridian Health, which has four hospitals ranked among the top 10 in New Jersey according to U.S. News & World Report – including No. 1 ranked Hackensack University Medical Center - more than any other network in the state. Robert focused on aggressive expansion of the Hackensack University Network before its merger with Meridian Health. As Co-CEO, Robert concentrates on innovation and leading partnerships, including launching New Jersey’s first private medical school with Seton Hall University and a historic partnership with Memorial Sloan Kettering Cancer Center.
Robert C. Garrett is Co-CEO of Hackensack Meridian Health, which has four hospitals ranked among the top 10 in New Jersey according to U.S. News & World Report – including No. 1 ranked Hackensack University Medical Center - more than any other network in the state. Robert focused on aggressive expansion of the Hackensack University Network before its merger with Meridian Health. As Co-CEO, Robert concentrates on innovation and leading partnerships, including launching New Jersey’s first private medical school with Seton Hall University and a historic partnership with Memorial Sloan Kettering Cancer Center. John K. Lloyd is Co-CEO of Hackensack Meridian Health, one of the largest, most comprehensive health networks in New Jersey, which includes 13 hospitals, 28,000 team members, more than 6,000 physicians and over 140 patient care locations across the state. John has focused much of his career on developing a full continuum of care – long before national health care reform mandated such changes. As Co-CEO, John oversees all non-acute care hospital businesses, including population health and the foundations. John’s expertise and vision have helped the network meet and exceed the challenges of health care reform.
John K. Lloyd is Co-CEO of Hackensack Meridian Health, one of the largest, most comprehensive health networks in New Jersey, which includes 13 hospitals, 28,000 team members, more than 6,000 physicians and over 140 patient care locations across the state. John has focused much of his career on developing a full continuum of care – long before national health care reform mandated such changes. As Co-CEO, John oversees all non-acute care hospital businesses, including population health and the foundations. John’s expertise and vision have helped the network meet and exceed the challenges of health care reform. Patrick R. Young is president of Population Health for Hackensack Meridian Health, where he leads the Population Health division and is responsible for accelerating the development of strategic priorities related to health care reform; population health management; Meridian’s Medicare Shared Savings Accountable Care Organization; Hackensack Meridian Health Partners, Hackensack Meridian Health’s clinically integrated network; health insurance partnerships; as well as overseeing Managed Care.
Patrick R. Young is president of Population Health for Hackensack Meridian Health, where he leads the Population Health division and is responsible for accelerating the development of strategic priorities related to health care reform; population health management; Meridian’s Medicare Shared Savings Accountable Care Organization; Hackensack Meridian Health Partners, Hackensack Meridian Health’s clinically integrated network; health insurance partnerships; as well as overseeing Managed Care.